

Abstract
Background: Recent studies (Coombs et al., Cell Stem Cell 2017) have identified presence of clonal hematopoiesis of indeterminate potential (CHIP) in samples of solid tumors. CHIP is more prevalent among cancer survivors who subsequently develop therapy-related myeloid neoplasm (Gillis et al., Lancet Oncol 2017; Takahashi et al., Lancet Oncol 2017; Gibson et al., J Clin Oncol 2017). However, the relationship between CHIP and exposure to myelotoxic chemotherapy delivered as part of treatment for solid tumor is uncertain. We hypothesized that CHIP is more prevalent among recipients of myelotoxic chemotherapy compared with age-matched population.
Methods: In this prospective, cross-sectional study, we collected peripheral blood samples from survivors of breast cancer or lymphoma who had received anthracycline- and/or alkylator-containing chemotherapy as part of their curative cancer therapy. All subjects had to be clinically free of cancer, and not have any hematologic disorders or unexplained cytopenias. We recruited patients age 50 to 70, because according to published population datasets (Jaiswal et al. and Genovese et al., NEJM 2014) in a cohort with mean age of 60 the expected CHIP prevalence would be about 5%. To minimize any potential contamination by circulating tumor cells, we isolated genomic DNA from purified CD45+ cells. We determined presence of CHIP by next-generation sequencing using an Illumina TruSeq Custom Amplicon kit (MiSeq V2.2). The assay targeted 757 coding exons of 96 genes commonly mutated in hematologic malignancies, including 20 CHIP-defining genes. To establish presence of CHIP, we required a known pathogenic variant with variant allele fraction (VAF) ≥ 2%. According to a pre-specified statistical plan, assuming one-sided alpha of 0.05, the study had 80% power to reject the null hypothesis of baseline CHIP prevalence of 5% in a cohort with sample size of 80.
Results: Among 80 enrolled subjects, median age was 62 years (interquartile range, 56-67). There were 78% women, and 88% of subjects were white non-Hispanic. Patients had received doxorubicin- and/or cyclophosphamide-containing adjuvant or curative chemotherapy for breast cancer (56%) or lymphoma (44%). Median time from completion of chemotherapy to enrollment was 27 months (interquartile range, 11-59).
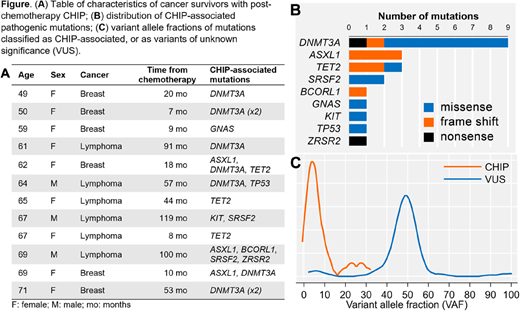
We have completed sequencing of 72 samples (updated analysis will be provided at the meeting). Mean coverage depth was 1418x (±224), and ≥200x coverage was achieved in a mean 91.4% (±1.8%) of target amplicons. We detected CHIP in 12 subjects (17%; binomial 95% confidence interval: 10-27%; P=.0002 for the null hypothesis test of 5% prevalence). Mean VAF for the CHIP mutations was 5.3% (range, 1.4% to 29.9%), and patients had up to 4 CHIP-associated mutations (Fig. A). The CHIP-associated mutations had a typical distribution with most common mutations in DNMT3A, ASXL1, SRSF2, and TET2 (Fig. B). There was only 1 TP53 mutation, previously suggested to associate with exposure to chemotherapy (Coombs et al., 2017). Potentially germline variants of unknown significance (VUS) were found in 78% of patients, at mean VAF 49% (Fig. C), most commonly in ATM (12%), NOTCH2 (7%), BCORL1, and DNMT3B (6% each). Additionally, 2 patients had low-VAF variants suspicious for CHIP: ATM c.6059G>A (3.0%); PRPF8 c.790T>C (VAF 2.3%). Presence of CHIP was not significantly associated with age (within the narrow age range in the study cohort), sex, race, type of cancer (breast or lymphoma), count of white cells, red cells, platelets, or time elapsed from completion of chemotherapy.
Conclusions: We have detected a significantly increased, more than 3 times the expected value, prevalence of CHIP among cancer survivors who had received myelotoxic chemotherapy. However, the distribution of mutations was typical for CHIP, without previously suggested over-representation of TP53. Further research is ongoing to determine whether presence of CHIP is related to a direct mutagenic effect of chemotherapy or competitive advantage of pre-existing CHIP clones after the hematopoietic stress of chemotherapy. Our data indicate that an affordable next-generation sequencing screen may be useful for detection of CHIP in cancer patients who are planning adjuvant chemotherapy, or as a surveillance tool after such therapy, to predict the risk of a therapy-related myeloid neoplasm and optimize personalized treatment strategies.
Olszewski:TG Therapeutics: Research Funding; Genentech: Research Funding; Spectrum Pharmaceuticals: Consultancy, Research Funding. Kim:Aushon Biosciences: Consultancy; LabCorp, Inc.: Consultancy; Papgene, Inc: Consultancy. Fenton:Astellas Pharma US: Other: Spouse employment. Reagan:Alexion: Honoraria; Takeda Oncology: Research Funding; Pfizer: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal